Kornilova L.N., Ekimovskiy G.A., Naumov I.A., Glukhikh D.O., Khabarova E.V.
The current methods of diagnostics of vertigo, dizziness and balance disorders entail significant financial and time expenses and can be applied exclusively in specialized hospitals possessing high-capacity diagnostic equipment such as magnetic resonance imaging (MRI), computer tomography (CТ), electroencephalography (EEG) etc.
 |
 |
 |
| Anamnesis and neurologist examination | Videooculography and videonystagmography | Caloric tests |
 |
 |
 |
| Rotary tests (vestibulometry chair and the centrifuge) | Tomography (neuro-imaging) | Galvanic vestibular stimulation |
Fig. 1 The most common methods to study and assess the vestibular system
The existing large financial and temporal expenses and technical difficulties inspire designing and development of more available hardware-software complexes and methods to objectify subjective vertigo/dizziness complaints, as well as to do initial differentiation of their cause already at the stage of primary health care.
Actual task is the creation of an expert-diagnostic computerized method and portable hardware-software complex which allow to receive a primary objective, reliable information about the state of the vestibular system based on characteristics of spontaneous eye movements and oculomotor reactions induced by vestibular and visual stimuli.
Fig. 2. Hardware-software complex “OCULOSTIM-CM” for objectification of systemic (vestibular) vertigo and non-systemic dizziness and differentiation of vestibulopathies of various genesis
Laboratory of Vestibular Physilogy at the SSC RF – IBMP RAS has developed a complex computerized method of vertigo/dizziness diagnosis, therapy and prevention that has no clinical analogs or references in Russian and international literature.

Fig. 3. The computerized method of comprehensive assessment of the state of vestibular function, intersensory interactions and visual tracking (Kornilova L.N. et al., Russian Federation patent #2307575, 2007)
In cooperation with LLC Medical Science Company “STATOKYN” and LLC Science and Production Association “INNOVATIVE MEDICAL TECHNOLOGIES” the methodology developed by laboratory of vestibular physiology was implemented in specially developed, portable mobile hardware-software complexes (HSC) “OCULOSTIM-CM”, “SENSOMOTOR” and “VIRTUAL” (the last one for using it abord the ISS in the space experiment) composed of:
- PC / notebook (for doctor) + projector / 2-nd widescreen monitor (for subject) for presentation of various visual and/or vestibular stimulation, and real-time control of received results with possible biofeedback.
- EOG-recorder – a special digital DC-device to record eyes (4-channel EOG) and head movements (3D angular velocity and linear acceleration sensors).
- Joystick to record hand movements in studying of visual-manual tracking and to record illusory reactions in studying of vections.
- Software – stimulation, registration of physiological signals, centralized storage and processing of data received.
 |
 |
Fig. 4. Examination on the HSC “OCULOSTIM–CM”
The created complexes allow to study:
- spontaneous eye movements (SpEM) with open and closed eyes;
- visually-induced oculomotor reactions – visual tracking (including smooth pursuit, fixation saccades and gaze holding) with and w/o additional visual noise/interference (retinal optokinetic stimulation (ROKS) ;
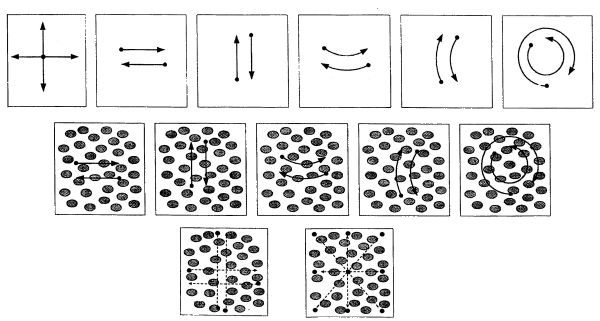
Fig. 5. Visual tests of the HSC “OCULOSTIM-CM”
- vestibular-induced oculomotor reactions;
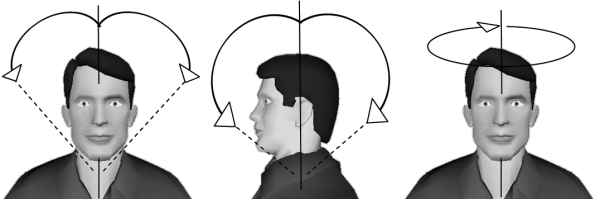
Fig. 6. Vestibular tests of the HSC “OCULOSTIM-CM”
- oculomotor reactions induced by combined visual and vestibular stimuli.
Under complaints of the patient and his medical history, the optimum course of diagnosis and appropriate diagnostic tests are selected (Fig. 7).
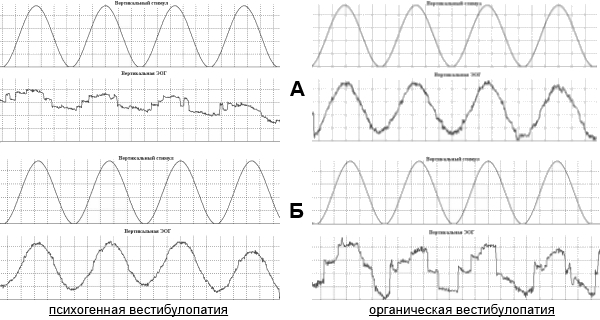 |
Fig. 7. Smooth tracking w/o (А) and with additional ROKS (Б) in patients with various types of vestibulopathy:
left part of the figure – patient with psychogenic vestibulopathy, right one – patient with organic vestibulopathy
Thus, developed methodology and computerized tests of the HSC “OCULOSTIM–CM” allows to study:
- spontaneous eye movements;
- nystagmus (spontaneous, optokinetic, vestibular etc.);
- visual tracking (static and dynamic saccades, gaze fixation and gaze holding, smooth pursuit);
- illusory reactions (vections);
- perception of a subjective visual vertical;
- static torsional otolith-cervical-ocular and otolith-ocular reflex (using additional videooculography complex);
- dynamic vestibular-ocular reactions and vestibular reactivity.
All tests can be carried out with and without (clear background) additional retinal optokinetic stimulation.
The next parameters are evaluated during processing of EOG, VOG and head movement data:
- amplitude and velocity of compensatory ocular counter-rolling during active head movements (rotations), the ratio of eye to head velocity (gain of vestibular-ocular reflex – gVOR);
- amplitude, velocity, time and frequency parameters of nystagmic reactions (relative duration of nystagmus as a ratio of total nystagmus duration to the overall test time, nystagmus frequency, quick phase amplitude, slow phase velocity etc.);
- latency and total reaction time, amplitude and velocity of fixations saccades and smooth pursuit (including efficiency coefficient – ratio of amplitudes of fixation saccades and stimulus movement, gain of smooth pursuit – ratio of the velocities of smooth pursuit and stimulus movement, percentage and amplitude of corrective saccades).
For each parameter characterizing the state of vestibular function and visual tracking there are evaluated various statistical characteristics (mean, variance, coefficient of variation etc.). Quantitative assessment and comparative analysis of the parameters are carried out by parametric and nonparametric methods of variance and correlation analysis. In all cases when statistical hypnotizes are used (normality of the distributions, homogeneity (equality) of variances, the reliability (significance) of differences) critical significance level α is 0.05.
In recent years, specialists of Laboratory of Vestibular Physiology are working on: a) the definition of reliable diagnostic criteria for differential diagnosis of vestibular disorders of different genesis based on assessment of characteristics of oculomotor reactions, b) and on the analysis and development of diagnostic criteria for differential diagnostics of changes in the vestibular-visual system for clinical patients with vestibulopathies and for cosmonauts.
This studies employs a well-known method of mathematical statistics – discriminant analysis that allows to differentiate (classify) subjects by certain criteria (discriminant variables). Discriminant analysis is used to attribute a person to the healthy group or a group of one or another vestibulopathy (peripheral, central, psychogenic, functional).
The developed hardware-software complexes “SENSOMOTOR”, “VIRTUAL”, “OCULOSTIM” and clinically-modified (CM) “OCULOSTIM-CМ” has been successfully tested and approved at the leading medical and research centers:
- State scientific center of the Russian Federation – Institute of BioMedical Problems of the Russian academy of sciences (IBMP)
(Department of Sensorimotor Physiology and Prophylaxis) - State Organization “Yu.A. Gagarin Research & Test Cosmonaut Training Center” (GCTC) (as part of the pre- and postflight examinations of cosmonauts)
- I.M. Sechenov First Moscow State Medical University (Department of Neurology and Department of Vegetative Nervous System Pathology)
- Clinical hospital № 83 of the Russian Federal Biomedical Agency (Center of Neurology and Neurorehabilitation)
- Federal Scientific Clinical Center of Otorhinolaryngology
- A. Vein Clinic for Treatment of Headache and Autonomic Disorders
- Special nursery school № 27 for children with visual impairments (Gomel, Belarus)
- Moscow Municipal Psychology Teaching University
HSC “OCULOSTIM–CM” received approval and is successfully used in:
- clinical practice (rehabilitation, neurology, otorhinolaryngology, ophthalmology);
- occupational selection and medical control (including the ISS-cosmonauts, highly-skilled sportsmen);
- scientific experiments and research studies (“dry” immersion, hypokinesis, bed-rest);
- evaluation of the effectiveness of pharmacological medicine (betahistine etc.);
- rehabilitation after neurologic diseases and traumas.
Some data obtained in the studies with the use of the HSC “OCULOSTIM-CM” are presented below.
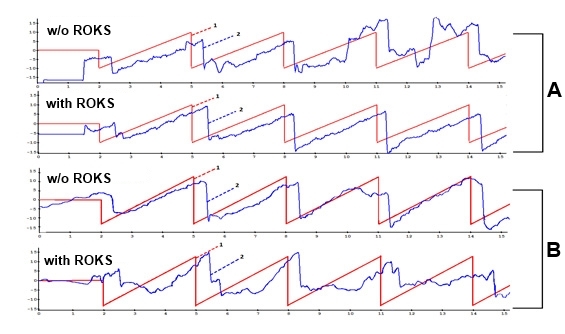
Fig. 8. Fragments of native curves of tracking of linear stimulus by patients with different types of vestibulopathies
А – a patient with psychogenic vestibulopathy, B – a patient with peripheral vestibulopathy,
1 – visual target (stimulus), deg.; 2 – eye movement (EOG), deg.
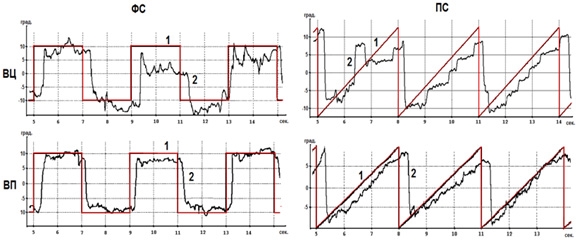
Fig.9. Fragments of native curves of tracking of saccadic and linear stimuli by patients with different types of vestibulopathies
ВЦ – central (cerebral) vestibulopathy; ВП – peripheral vestibulopathy;
ФС – fixation saccades; ПС – smooth pursuit
1 – visual target (stimulus), deg.; 2 – eye movement (EOG), deg.
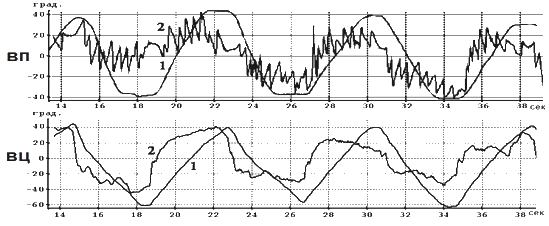
Fig. 10. Fragments of native curves of oculomotor reactions during active head movements (vestibular reactivity) by patients with different types of vestibulopathies
ВП – peripheral vestibulopathy, ВЦ – central (cerebral) vestibulopathy
1 – head movement, deg.; 2 – eye movement (EOG), deg.
To validate the proposed methods to vertigo/dizziness objectification and differentiation of vestibulopathies and to test the HSC “OCULOSTIM-CM” there was performed a control study with a group of patients whose clinical diagnoses were known from the results of neuro-visual and clinical survey (MRI etc.). The accuracy of classification of healthy people was 95.5%, for patients with organic (central and peripheral) vestibulopathies it was 81.0% and for patients with psychogenic vestibulopathies – 70.8%.
The developed methodology and innovative hardware-software complexes can be applied in:
- expert diagnostic assessment of the vestibular function and objectification of complaints of vertigo, dizziness and equilibrium disturbances using specially developed computerized tests based on registering of spontaneous, visually- and vestibular-induced eye movements;
- formation of reliable diagnostic criteria for differential diagnosis of vestibular disorders of different genesis using analysis of characteristics of eye movements;
- detecting the presence and type of vestibulopathies in different groups of patients in the clinic and in extreme (special) professions;
The studies were carried out under the Russian Space Research Program (1990-2000), and within research projects (6001/4, 6001/5, 6001/6, 6001/7) supported by Task Program «Fundamental Sciences – For Medicine» within the Fundamental Research Program at the Presidium of Russian academy of sciences (2009-2013).
For joint participation in this work, the authors thank the academics Vein A.M. and Palchun V.T.; professors, doctors of medical sciences Solovieva A.D., Zaitseva O.V., Shvarkov S.B., Filatova E.G., Fedorova V.I., Akarachkova E.S.
Special thanks are extended to the neurologist, former employee of the laboratory Temnikova Valentina V.
Having the positive comments from Russian and foreign colleagues on the published results of our studies we conceive that they should be continued. Results obtained by using the computerized methods are needed for operative diagnosis and effective, adequate therapy, and for minimization of using of additional neuro-visual (imaging) and instrumental means for examination/survey of patients on the pre-symptom (subclinical) or remission phases.