RESULTS OF STUDIES IN 1984-2014
Kornilova L.N., Naumov I.A., Glukhikh D.O., Ekimovskiy G.A.,
Sagalovich V.N., Khabarova E.V., Pavlova A.S.
The beggining of human spaceflights gave science tasks to study causes and mechanisms of atypical perception and sensorimotor reactions associated not only with early adaptation and long exposure to weightlessness (microgravity) , but also readaptation on return to Earth. Understanding of phenomenology and mechanisms of the sensory disorders was necessary for the development of methodology of prediction and correction of these atypical reactions during spaceflight.
It was found out that almost every cosmonaut reported a number of specific adverse sensory reactions, particularly illusions of spatial position, vertigo/dizziness, difficulties with fixation on and pursuit of visual objects within the field of vision. This condition is felt as discomfort especially with additional autonomic (vegetative) symptomatology. The arising sensory disorders have negative effects on cosmonaut’s health and ability to perform their professional tasks qualitatively in microgravity.
On Earth, spatial perception and orientation are controlled by the gravity-independent (ocular, hearing, smelling) and gravity-dependent (vestibular, support) systems. The gravity-dependent systems, adjusted to function in the Earth’s gravity, act as triggers of atypical reactions in altered gravity. Nature of these reactions, their intensity and dynamics are determined by integrative structures of the central nervous system (CNS) which perform multisensory convergence of afferent signals of various modality and provide the functioning of the vestibular and visual system.
The first vestibular studies onboard the USSR/Russia space vehicles “Soyuz” and orbital stations “Salyut 3-7″ brought to light that in addition to complaints of orientation illusions, vertigo/dizziness, nausea and vomit cosmonauts experienced also discoordination and difficulties with fixation on and tracking visual objects within the field of vision.
Analysis of cosmonauts’ subjective complaints showed that atypical sensory reactions in microgravity are a direct consequence of sensory shifts and ensuing sensory adaptation. Adaptation to microgravity hinges on two parallel processes, i.e. modification of the habitual phylo- and ontogenetically evolved interaction of sensory systems and establishment of new sensory interactions in the CNS. Atypical perception, sensory, sensorimotor and autonomic reactions developing at the beginning of adaptation to microgravity reflect changes in functioning of the physiological systems responsible for collecting and processing of sensory information and formation of integrated perception-motor reactions. Inherent to the adaptation to microgravity symptomatology of atypical reactions is nothing else but a natural reaction of organism to a new environment, i.e. a special “space” form of the adaptation syndrome (SAS) associated with shifts in the level and nature of vestibular and support afferentation, changes in the nature of intersensory interactions and central integration of sensory inputs. When reactions typical to SAS reach clinical level and cause critical detriment of professional and physical performance, such state will be diagnosed as space motion sickness (SMS). SMS is a state when normal physiological adaptation degrades into decompensation.
Retrospective analysis of the studies of illusory reactions both spontaneous and induced by optokinetic stimulation (OKS) carried out onboard the “Salyut” and “MIR” stations within the Russian experiment “ANKETA” with participation of Russian and international crewmembers, and as part of the Russian national program (experiments “OPTOKINEZ”, “OCULOSTIM”), Russian-Bulgarian (“LABIRINT”) and Russian-Austrian (“OPTOVERT”) programs made possible the first systematization of phenomenology and classification of atypical perception and vestibular-sensory reactions in microgravity.
Tolerance of spaceflight was estimated based on subjective data from 104 cosmonauts who participated in ANKETA and 17 cosmonauts who participated in other space experiments. Answers to questionnaires, comments in diaries, logbook entries and dictaphone records were made starting from 3rd day of spaceflight (first day of ISS mission) till completion of adaptation to microgravity, then before and after using of in-flight countermeasures, in all cases of ailment, and on return to Earth. Results of the experiments were subject to mathematical statistical processing using correlation analysis.
Russian research of spatial perception, spontaneous and visually-induced illusory reaction in microgravity and during readaptation to terrestial conditions
1. Spatial perception
Analysis of questionnaires and dictophone records within the experiment “ANKETA” has shown that 98% of cosmonauts developed some degree of illusory reactions and signs of spatial disorientation. When vision was “switched off” it impaired spatial orientation and perception. Full darkness or free floating inside the space vehicle cabin with closed eyes led to a partial or complete disorientation. 41% of cosmonauts mentioned that they could not in the least estimate height in microgravity. All environment inside and outside the vehicle was perceived in terms of distance and depth rather than height. Cosmonauts differed in their sensation of the surrounding and own positioning in microgravity.
Most of the cosmonauts (58%, among which 82% were pilots) formed perception of space and their own position with the help of visual cues (visually orienting type of people). Viewing a mate floating with his head over heels or visual objects where they cannot be from the earthman’s perspective caused discomfort in these cosmonauts. The number of those who experienced vestibular disorders in the period of adaptation to microgravity reached 60% of the group. The second group of cosmonauts (34%, among which 18% were pilots) oriented in space and could locate themselves mainly relying on their internal body coordinates (type of people orienting by internal body coordinates). This category of cosmonauts always thought that the top is where the head was pointed to and, therefore, the floor was what they touched with their feet. Motion sickness was developed by 9% of the group members. There was a small group of cosmonauts (8%) who could not explain what helped them with spatial orientation and perception. Evidence for orientation dependence of cosmonauts in flight suggested that atypical vestibular reactions in microgravity had different genesis and were determined either genetically or professionally, and by the specific weight of one or another of sensory inputs to construction of spatial image.
Studies of accuracy of perception of subjective visual vertical (SVV) in the dark with stationary and moving up and down OKS conducted in the period of adaptation to microgravity pointed to the growth of the error of SVV perception by 8 to 18°, particularly following OKS and on the background of a fixed graphic. Unlike the preflight results, inflight errors shifted leftward irrespective of test conditions. With extension of the period in microgravity, the SVV error, as a rule, exceeded the physiological norm.
Estimation of the SVV error on days 1 and 2 after landing showed that accuracy of SVV perception degraded in almost all cosmonauts in every position, i.e. sitting, lying on the right or left side. Error value was particularly significant in the side positions. In these positions, most often asymmetry jumped together with change in its trend as compared with baseline data; also, 18% of cosmonauts flown in long-term missions changed the so-called Aubert phenomenon for the Muller one, i.e. the SVV error aligned with the body inclination.
2. Spontaneous illusory reactions
The earliest manifestation of microgravity was appearance of orientation illusions (98%). Illusory sensations showed themselves suddenly right at the time of transition to microgravity and gradually fainted away over few hours and even minutes. However, some cosmonauts had them persistently when closing eyes for 14 to 30 days (19%) or even throughout the whole mission (96 to 365 days) (7% of cosmonauts). Spontaneous orientation illusions were amplified and grew worse with closed eyes.
2.1. Kinetic illusions (rotatory and linear)
Kinetic illusions were characterized as follows (Fig. 1):
- sensation of self-rotation around the frontal (Y) axis in the saggital plane forth-down, more frequently back-down (dynamic pitch illusions);
- sensation of self-rotation around the frontal (Y) axis followed by rotation around the longitudinal (Z) axis typically clockwise (combined dynamic pitch and yaw illusions);
- sensation of self-rotation around the saggital (X) axis in the frontal plane, often rightward combined with the sensation of clockwise rotation around the longitudinal (Z) body axis (combined dynamic roll and yaw illusions).
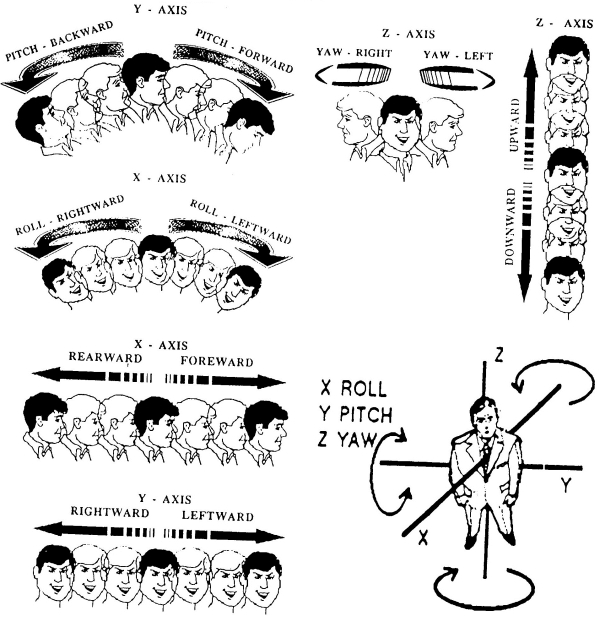
Fig. 1. Types of illusions in spaceflight: rotary, linear, static, combined
There were numerous observations of rotatory illusions combined with linear, i.e. the sensation of linear top-down movement along the body longitudinal (Z) axis (“bob” illusions) together with linear clock- and counterclockwise movement along the body frontal (Y) axis (“heave” illusions).
Prevailing kinetic illusion was pitch (71%) per so and in combination with other movements.
2.2. Coordination illusions
As a rule, kinetic illusions turned to the body coordination ones:
- positional head-down illusion (inversion);
- body inclination to the left or, more often, right (static roll)
- body inclination forward or, more often, backward (static yaw).
Illusions of inversion prevailed (72%).
2.3. Proprioceptive and other illusions
Along with illusions of movement, also reported were proprioceptive illusions (9%) during and after stay in microgravity. Some said they had sensed “a falling wall” they tried to hold back with their hands and the floor streaming away under their feet. A few cosmonauts (7%) reported the illusion of misplaced body parts (“I thought my hands were down but they were up instead”, “you feel like you sit crooked but in fact lye straight in your sleeping beg”).
There were cosmonauts (21%) who found it difficult to envelop with the gaze surrounding things and indicators on the control panel and encountered with the illusion of control board “approaching” or “shifting” horizontally or vertically, but more often upward. 32% of cosmonauts reported illusion of nearby things jerking at the time when they were engaged in visual tasks that required head movements (oscillopsia).
In the course of prolonged exposure to weightlessness the illusory reactions episodically returned after sleepless night, strenuous motor activity or heavy stress loads.
By the rate of occurrence illusions can be ranked as follows: combined – 41%, coordination (inclination of the self or surrounding things) – 31%, kinetic (rotary-linear movement of the self or surrounding things) – 28%.
2.4. Vection illusions
Studies of vection illusions induced by linear and sinusoid vertical OKS for the first time has shown such unique microgravity phenomenon as vection inversion when direction of illusion and OKS was unidirectional rather than in antiphase (Fig. 2).
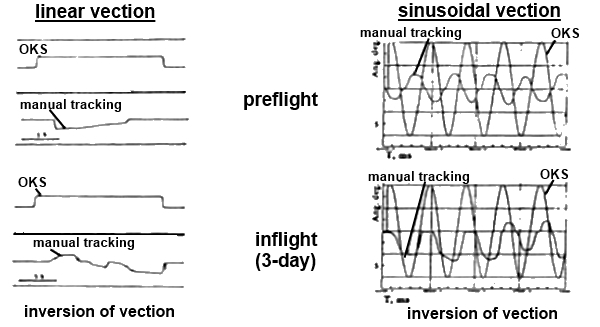
Fig. 2. Vertical vection illusions (vection inversion) in microgravity:
OKS – optokinetic stimulation, MT – manual tracking (hand points to direction of illusion)
3. Correlation between illusory, sensorimotor and autonomic reactions
By the end of the first day of spaceflight but commonly on the second day reflex perceptive-motor reactions were replaced in all cosmonauts by the sensation of blood rush to the head and heaviness in the head; some cosmonauts developed headache. Other symptoms occurring in this period included stuffiness in nose, injection of vessel sclera and progressive face puffiness. Noteworthy is the fact that some cosmonauts (11%) attributed illusory sensations to the blood rush to the head at the beginning of adaptation to microgravity. Others (23%), having the sensation of blood rush, developed also autonomic reactions, i.e. change in integument color (turning red oftener than pale), cold sweat, belching, heaviness in the epigastric region, hypersalivation, loss of appetite, nausea and vomit, sometimes multiple. Vomit was usually sudden without preceding prodromal nausea. Intervals between attacks were up to 3 hours long. These sensations could remain from several minutes and hours up to 6-14 days; two cosmonauts had to tolerate them for 30 days in orbit. Typically, gastrointestinal symptomatology appeared and sustained between 30 and 48 hours of the spaceflight. Performing of critical flight operations eased the discomforting symptoms and distracted cosmonauts from unpleasant sensations. Sleep improved general condition significantly and decreased discomfort.
Comparative analysis of illusory and autonomic reactions in weightlessness showed that atypical vestibular reactions take place in a strict sequence. Whereas illusions appeared almost immediately, autonomic phenomena came in a little while, i.e. at the end of the first or second day on the orbital station. Time gap between the illusory and autonomic reactions may mean that they are not connected directly as was confirmed by the results of correlation analysis (r = 0.26; p < 0.05).
In addition to illusionary reactions, 72% cosmonauts faced difficulties with tracking of and gaze holding on a moving target, and effects of discoordination such as a missing at the attempt to catch an object or head bumps into wall panels when floating about the station. Mathematical analysis established a position correlation (r = 0.74; p < 0.05) between orientation illusions and disorders in oculomotor reactions.
4. Factors provoking appearance and amplifying of illusory and autonomic reactions
The majority of cosmonauts (68%) are unanimous in the opinion that high motor activities, especially sharp/abrupt head and body movements on the initial days in flight were the main stress factor provocative of illusionary and autonomic reactions. As a rule, transition from the “Soyuz” vechicle to the orbital station aggravated both the illusory and autonomic reactions. Movements in the saggital and frontal planes were the most dangerous.
According to 21% of cosmonauts, illusory and autonomic reactions were initiated by optokinetic stimulation and lack of the normal sense of support as well as of top/down awareness. In view of many cosmonauts, watching objects moving on Earth or air out of window made illusory and autonomic reactions much stronger. Some cosmonauts (11%) experienced illusory and autonomic reactions also with the head fixated motionlessly and associated them with blood rush to the head at the beginning of adaptation to microgravity.
5. Patterns of sensory systems adaptation/readaptation
Body adaptation/readaptation to factors of the spaceflight may proceed on one of three patterns defined by the length and intensity of illusory and autonomic reactions:
- conditionally resistive – no vegetative or sensory discomfort; illusory reactions are mild and short (second and minutess) (21%);
- violant – pronounced illusory, discoordination and/or autonomic reactions persisting 1-3 days (54%);
- torpid – weak illusions and/or symptoms of autonomic discomfort persisting 14 or more days (25%).
In repeated spaceflights, sensory adaptation on the first pattern was observed in 61%, second – 32% and third – 7% of cosmonauts.
Return to Earth was accompanied by recurrence of spatial, sensorimotor and autonomic disorders. Spatial illusions always developed in those cosmonauts who had suffered them in microgravity. In contrast to spaceflight, during the initial hours on Earth illusions of self-rotation or rotation of environment were instigated mainly by head movements in the horizontal plane around the longitudinal body axis (“yaw”). Some cosmonauts had illusions only in a certain head position, the so-called positional kinetic illusions (12% of cosmonauts – rotary and 8% – linear illusions). Postflight 7% of cosmonauts complained of impaired spatial perception of body position, that is the horizontal position was taken for inclination below the horizon by 10-15 degrees.
Autonomic and sensorimotor disorders were always more intensive postflight than inflight and developed both in those who had experienced them in orbit, and those (11%) who, according to verbal reports, had not had these problems during the spaceflight.
6. Periods and phases of dynamics of adaptative neurosensory processes to prolonged exposure to weightlessness
Analysis of cosmonauts adaptive reactions to long-term microgravity showed that in the history of the Russian manned space program there had never been a case when a cosmonaut who felt vestibular discomfort was unable to adjust to microgravity. When adaptation was completed, cosmonauts could make all kinds of movement which commonly did not provoke unpleasant vestibular reactions. However, attention should be paid to the fact that some cosmonauts (24 of 104) on long-term missions (75-438 days) had episodes of slight vestibular discomfort (vertigo/dizziness and nausea) in consequence of active locomotion; two cosmonauts experienced discomfort even at rest.
Data collected in and after flight shed light on periods and phases of adaptative neurosensory processes. In the course of time, atypical perceptive, sensorimotor and autonomic reactions during early adaptation/readaptation faded away as a result of adaptive/readaptive changes in the CNS. To perform motor acts correctly and to sucessfully orient in space in weightlessness, CNS blocks abnormal vestibular inputs (central vestibular deafferentation) and forms new intersensory relations. However, based on the results of studies in long-term microgravity, these new intersensory relations were fairly unstable and could be easily broken by additional unfavorable factors. Therefore, character of changes in sensory interactions was transitory all through the whole spaceflight that is dominance passed on from adaptation to readaptation. Readaptation also was a wave-like process.
Russian and joint international researches of the vestibular function and visual tracking in weightlessness and during readaptation to Earth
Considering the dependence on the gravitation factor, large scope of vestibular functional relations and obligatory involvement of the vestibular system in whole-body reactions, many investigators associate the set of atypical sensorimotor reactions to microgravity with alterations in the vestibular function (otolith deafferentation, otolith-canals conflict, inter-labyrhinths asymmetry, intersensory mismatch, change in the labyrhinths internal environment due to the redistribution of body liquids in the cranial direction), and all functions based on vestibular afferentation. The standpoint of the primary role of the vestibular system in atypical reactions to the altered gravity is supported by resistance of people with non-functioning labyrhinth to the factors of parabolic flight, Coriolis and precession accelerations. We can assume that the vestibular apparatus acts as a trigger of the Space Adaptation Syndrome (SAS) and Space Motion Sickness (SMS) and that the CNS integrative structures determine the SMS intensity and nature. In their turn, the CNS structures carry out the multisensory converging of afferent inputs of varying modality and provide implementation of vestibular and other functions.
In this section, we present the results of national (USSR/Russian) experiments and experiments fulfilled in cooperation with international teams of reseachers. Studies in microgravity were made with the use of specially developed systems including: OPTOKINEZ for the Russian-Hungarian experiment of the same name (Hungarian co-investigator – Prof. G. Bodo), Zora for the Russian-Bulgarian experiment LABIRINT (Bulgarian co-investigator – Prof. V. Grigorova), DataMIR-Optovert for the Russian-Austrian experiment OPTOVERT (Austrian co-investigator – Prof. H. Muller), Videooculograph for the Russian-German experiment VOG (German co-investigator – Prof. A. Clarke), ASYMMETRY for the Russian-Slovak experiment of the same name (Slovak co-investigator – Prof. F. Glavachka) and BIOCONTROL for the Russian-US experiment of the same name (US co-investigator – Prof. P. Cowings). All information was digitized, filed and stored in PC memory and processed on return to Earth using specially developed software.
Studies onboard the orbital stations “Salyut-7″ and “MIR” involved 31 cosmonauts; 27 cosmonauts were on long-term missions (76-438 days) and 4, on short-term missions (7-9 days). 13 cosmonauts participated in experiments two and more times. Cosmonauts’ age ranged from 28 to 50 years. Each cosmonaut was tested on 30 and 10 days before launch (baseline data collection), inflight on days 2(3), 5(6) and 28(30), than once a month or two months till end of the spaceflight, postflight on days R+1(2), R+4(5) and R+8(9) and on R+14 and 19, if necessary.
In addition, 40 Russian crewmembers of the ISS long-term expeditions (starting from the ISS-3) were tested during the spaceflight (space experiment VIRTUAL, since ISS-37/38 expedition) and before and after spaceflight (science experiment SENSORY ADAPTATION). These cosmonauts were in weightlessness from 125 to 215 days (average period of stay aboard the ISS was approx. 175 days). Cosmonauts’ age ranged from 35 to 54 years averaging 45 years.
All cosmonauts had undergone extensive medical examinations (including examination by an ophthalmologist and neurologist), had normal vision with no oculomotor abnormalities, had no known clinical vestibular problems, and were not taking drugs which affect the nervous system. The study protocol (space experiment «VIRTUAL», science experiment «SENSORY ADAPTATION» and clinical-physiological assessment «Vestibular Function Check up») was reviewed and approved in advance by the Bioethics Board of the Institute of Biomedical Problems and Human Research Multilateral Review Board. All cosmonauts gave written, informed consent before participating in the experiment.
Oculograms were analyzed to determine:
- amplitude of the compensatory torsion ocular counter-rolling in the static position of the head after the tilt-to-shoulder;
- gain of the otolith-cervical-ocular reflex (gOCOR) – ratio of amplitude of the compensatory torsion ocular counter-rolling and head tilt angle;
- amplitude and velocity of compensatory eye movement during active head movements;
- gain of the vestibular-cervical-ocular reactions (gVCOR) – a ratio between velocity of head movement and velocity of the compensatory eye movement;
- latency, amplitude, velocity and frequency parameters of nystagmic reactions (amplitude of nystagmus quick phase ANy , velocity of nystagmus slow phase VNy, nystagmus frequency FNy);
- latency, amplitude and velocity parameters of visual tracking, including the efficiency ratio of fixation saccades (eFS) – ratio of amplitudes of eye (saccade) and stimulus movements; gain of smooth pursuit (gSP) – ratio of eye and stimulus velocities .
For each parameter characterizing the state of vestibular function and visual tracking there were evaluated various statistical characteristics (mean, variance, coefficient of variation etc.). Quantitative assessment and comparative analysis of the parameters are carried out by parametric and nonparametric methods of variance and correlation analysis. In all cases when statistical hypnotizes are used (normality of the distributions, homogeneity (equality) of variances, the reliability (significance) of differences) critical significance level α is 0.05.
The relationship between the vestibular input and visual tracking in microgravity was evaluated by parameters of the visual tracking following a series of active head movements (rotations) at 0.125 Hz.
To determine contribution of the tactile-support afferentation to modulation of the oculomotor reactions in microgravity, an additional support was created by fixation of the back and legs to the station wall using belts or the treadmill bungee cords generating axial loading (50% of body weight) to feet.
Spontaneous and vestibular-induced oculomotor reactions
Spontaneous eye movements (SpEM)
Preflight, with one exception all cosmonauts had stable oculograms. SpEM assessment on the first day in flight showed its increase in almost every cosmonaut in the form of drift and saccadic (primarily – square wave jerks) eye movements. Almost in half cases (42% of cosmonauts) in addition to increased SpEM there was also a spontaneous nystagmus (ANy = 3.7±0.3º; VNy = 6.3±0.8º/s; FNy = 0.5±0.04Hz) which was either vertical or combined horizontal+vertical. On 5-6 day inflight spontaneous nystagmus disappeared; however, in some cosmonauts the saccadic activity remained high.
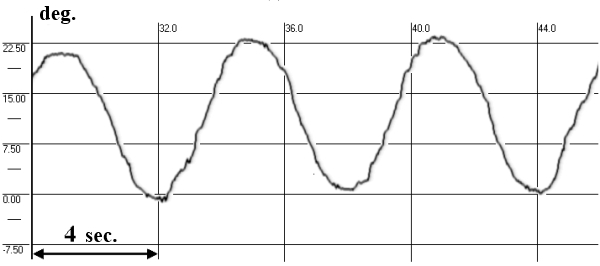
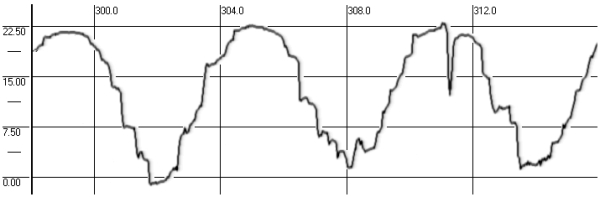
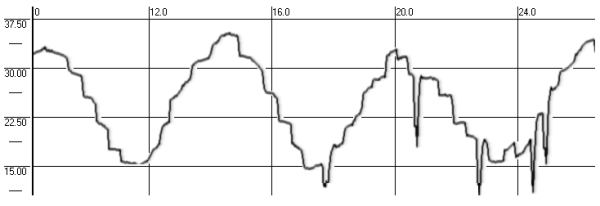
Further into spaceflight (starting from 60-day or sometimes 30-day) eyes got destabilized once and again as a result of increasing slow drifts, emergence of numerous saccades and a spontaneous nystagmus which were predominantly vertical (Fig. 3.).
preflight
inflight (3-day)
inflight (43-day)
postflight (R+2)

Fig. 3. SpEM before, during and after long-term spaceflight
Examinations on R+1(2) demonstrated normal SpEM in 36% of cosmonauts. Increased numbers of saccadic and drifting SpEM were found in 26% of cosmonauts, spontaneous nystagmus (ANy = 3.5±0.5°; VNy = 6.1±0.7°/s; FNy = 1.5±0.03Hz) and gaze-evoked nystagmus (ANy = 2.5±0.5°; VNy = 3.9±0.7°/s; FNy = 0.5±0.08Hz) were registered in 38% of cosmonauts. On R+8(9) SpEM were stable.
Static torsion otolith-cervical-ocular reflex (OCOR)
On Earth, head tilts to the shoulder as well as forward and backward movements give rise to compensatory ocular counter-rolling aimed to ensure gaze stability and adequate spatial perception. In microgravity OCOR was studied in 4 cosmonauts. In two of these 4 cosmonauts head tilt to the shoulder was never accompanied by the torsion otolith ocular counter-rolling throughout the whole spaceflight (expeditions with duration of 178 and 438 days). In a third cosmonaut eyes rolled in the same direction as head tilt (OCOR inversion, paradox OCOR); in a forth cosmonaut ОCOR decreased sharply.
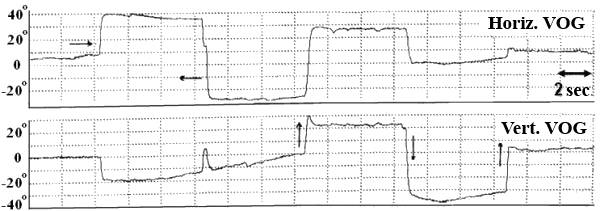
Post-flight OCOR was studied in 32 cosmonauts. On R+1(2) 30% of cosmonauts did not have the torsion compensatory ocular counter-rolling; 8% of cosmonauts had iversion of OCOR (eyes rolled in the same direction as head tilt ) (Fig. 4); in 37% of cosmonauts the amplitude of OCOR was reduced by 50%; in 25% of cosmonauts OCOR was practically normal. On R+8(9) amplitude of OCOR was close to baseline values.
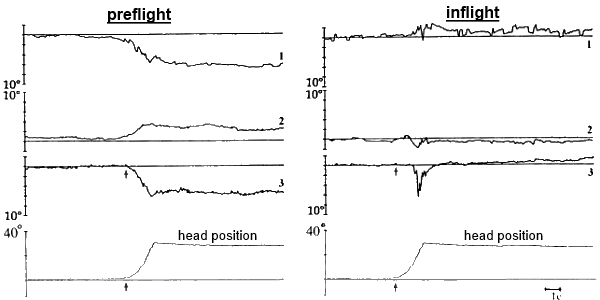
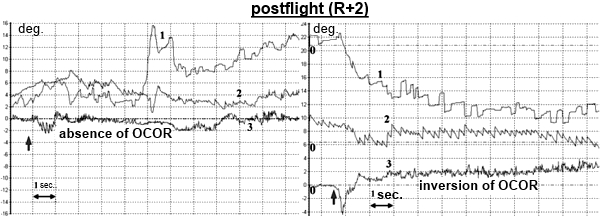
Fig. 4. OCOR before, during and after spaceflight:
1 – horizontal VOG, 2 – vertical VOG, 3 – torsional VOG,
↑ – moment of head tilt to the right
Dynamic vestibular-cervical-ocular reflex (VCOR) and vestibular reactivity (VR)
Dynamic vestibular-oculomotor reactions were induced by active head movements (rotations) in the horizontal plane within ±45° at 0.125 Hz. Head rotation was performed with eyes closed and open (in darkened goggles). Rhythm of head movement was set by a sound signal of varying frequency. Preflight, gain of the horizontal vestibular-cervical-ocular reactions (gVCOR) was within the normal range of 0.4-0.5 in all cosmonauts. Active head movement (rotation) with closed eyes generated single strokes of nystagmus.
During early adaptation to microgravity, in 47% of cosmonauts head rotation around the longitudinal body axis (horizontal VCOR) increased gVCOR to 0.6-0.7. Head velocity decelerated significantly and asymmetry of reactions was pronounced (52%). In the course of further adaptation to microgravity gVCOR returned to the baseline. After 60 days inflight (sometimes 30 days) 40% of cosmonauts showed reduction of gVCOR to 0.1; in 30% of cosmonaut – gVCOR dropped to zero and did not rise till end of flight (Fig. 5).
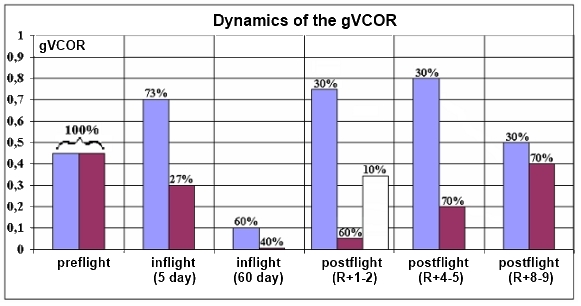
Fig. 5. Dynamics of gVCOR before, during and after spaceflight
Horizontal VCOR during the early adaptation to microgravity was distinguished by nystagmus superposition – the reaction of compensatory eye movements were accompanied by nystagmus. After 30 days inflight, the nystagmic reaction was not actually seen, unless head movements were performed with open eyes. After 60 days inflight active head rotation with closed eyes did not produce the nystagmus. 30% of cosmonauts also did not have the compensatory ocular counter-rolling.
Postflight, depending on the gVCOR value the cosmonauts were distributed into two groups. In one group (20% of cosmonauts) gVCOR increased to 0.7-0.8 immediately after landing (R+1-2). This increase was due to the deceleration of velocity of head rotation around the longitudinal body axis. In the other group (65%) gVCOR decreased sharply to 0.1-0.15 or was almost equal to zero because of the absence of compensatory ocular counter-rolling (no static component). In 15% of cosmonauts gVCOR remained within the baseline values.
The vestibular function postflight was characterized by the presence of nystagmus (ANy ~ 6°-10°; FNy ~ 2-4Hz) accompanied by a sharp decrease of the compensatory ocular counter-rolling (Fig. 6).
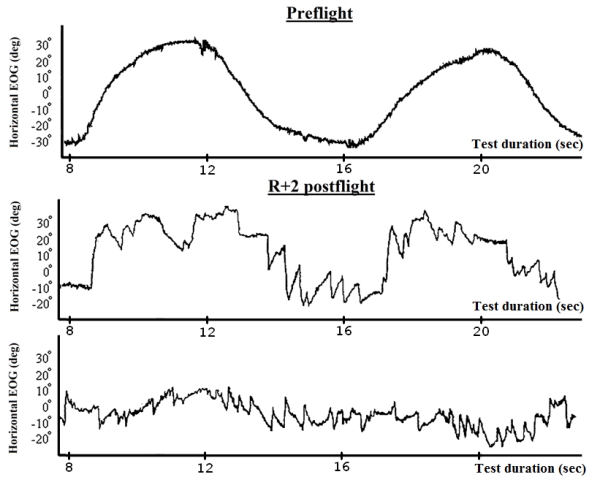
Fig. 6. The vestibular-cervical-ocular reactions before, during and after spaceflight
On R+8(9) the vestibular function was normal in 85% of cosmonauts.
Correlation analysis of changes in the functional state of the otoliths and semicircular canals has shown a negative correlation between parameters of OCOR and VCOR (r = -0.8; p < 0.05) which suggests a reciprocal interrelation of these reflexes and presence of an otoliths-canals conflict inflight and also during acute period of readaptation with central deafferetation of the otolith input. On R+8(9) the correlation coefficient between OCOR and VCOR acquired a positive value (r = 0.4) that may infer a normalization of the otolith input and regain of synergy in the interrelation of the otoliths and canals subsystems that had been observed in cosmonauts preflight.
Vestibular-optokinetic reactions in microgravity
In the early period of spaceflight, combined vestibular-optokinetic stimulation (head rotation around the longitudinal body axis at 0.125 Hz within ±45° with retinal OKS) induced predominantly oculomotor reactions of vestibular genesis. Studies performed at the end of adaptation (30 or 60 days of spaceflight) with simultaneous stimulation of the vestibular and visual systems resulted in weakening or disappearance of vestibular reactions and growth of optokinetic. This implied increase of significance of the visual input and decrease of significance of the vestibular input in formation/generation of oculomotor reactions to the combined vestibular-optokinetic stimulation.
Visually-induced oculomotor reactions
In weightlessness vestibular system (otolith receptors) is the trigger of atypical sensorimotor reactions, which may lead to less accurate visual and visual-manual tracking.
It is customary to assume that in microgravity the reliable source of information is visual input, as it does not belong to the gravity-dependent systems but is an organ for perception of visual objects. However, a question arises as to how fair this assumption if we consider that gravity-dependent and independent sensory systems interact closely in their functioning and character of these interactions determines gaze stability and accuracy of visual tracking. In this regard, more plausible seems to be the hypothesis about a limited reliability of the visual input as in microgravity, so also during readaptation to Earth’s gravity long-term spaseflights.
Accuracy of fixation saccades (FS)
Analysis of FS at the beginning of adaptation to microgravity showed that in the majority of cosmonauts (78%) percentage of additional corrective saccades increased from 3% (baseline) to 18.5% during horizontal pursuit and from 6% to 30% during vertical pursuit. Duration of reaction of stimulus’ acquisition and fixation (total reaction time) increased in 2.5-3 times; latency increased by 15-45% for horizontal and by 18-54% for vertical saccades (Fig. 7).
| preflight | inflight |
 |
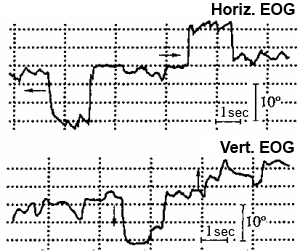 |
Fig. 7. Fixation saccades before and during spaceflight
Postflight dynamics of the parameters of horizontal and vertical saccades (latency, eFS, peak velocity, percentage of corrective saccades) was similar to dynamics during adaptation to microgravity (Table 1).
Analysis of FS at the beginning of postflight readaptation has shown a significant decrease of latency, amplitude and velocity parameters of saccades that partially reached the baseline values only by R+8(9) (Fig. 8).
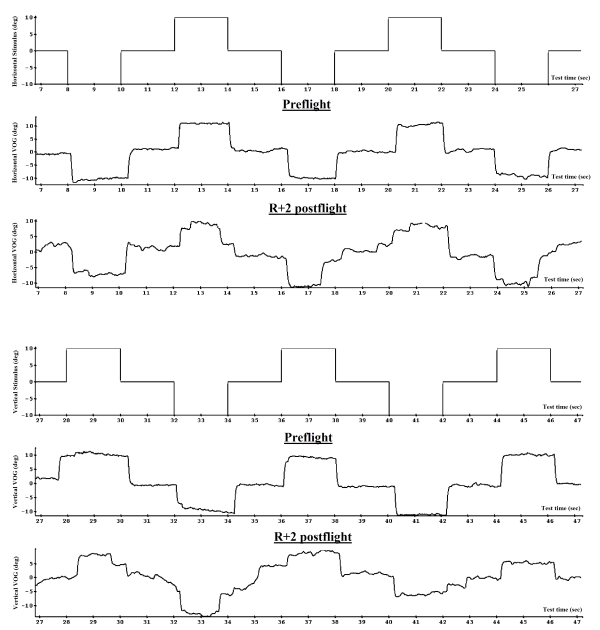
Fig. 8. Fixation static saccades before and after spaceflight (VOG)
Smooth pursuit (SP)
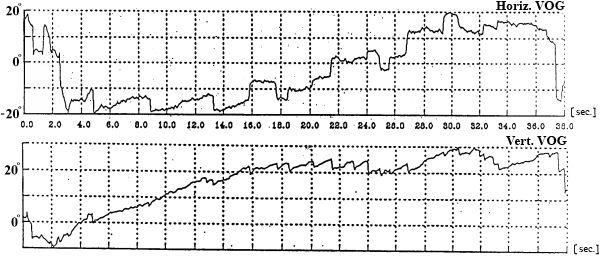
Analysis of SP of a linear and sinusoidal stimulus moving horizontally and vertically during the initial adaptation to microgravity revealed disorders in the SP function and also cases of full breakdown of the reflex (27% of cosmonauts). The eye was unable to pursue stimulus smoothly and switched to a different strategy, i.e. saccadic approximation (Fig. 9). Registered gaze movement was not smooth but step-by-step (a series of corrective saccades) in pursuit of a linear or sinusoidal stimulus. This change of pursuit strategy led to a sharp increase of duration of SP reactions (in 2-3 times). On completion of adaptation, tracking regained its smooth character; however, gSP (a ratio of eye and stimulus velocities) did not reach preflight level.
| preflight | inflight |
 |
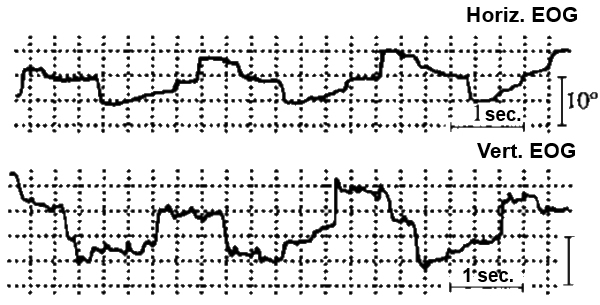 |
Fig. 9. Smooth pursuit before and during spaceflight
Changes in SP during postflight readaptation were similar to changes occurring in microgravity. As with OCOR, in some cosmonauts full recovery of SP was observed only by R+14(19) (Fig. 10 and 11). Pre- and postflight dynamics of gSP is shown in Table 1.
preflight
postflight (R+2)
postflight (R+5)
postflight (R+9)
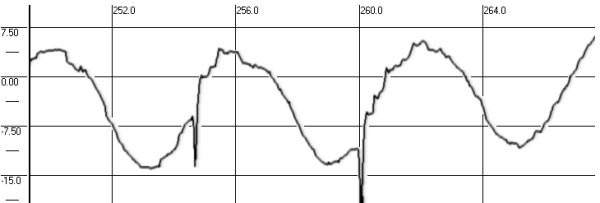
Fig. 10. Smooth pursuit before and after spaceflight (VOG)
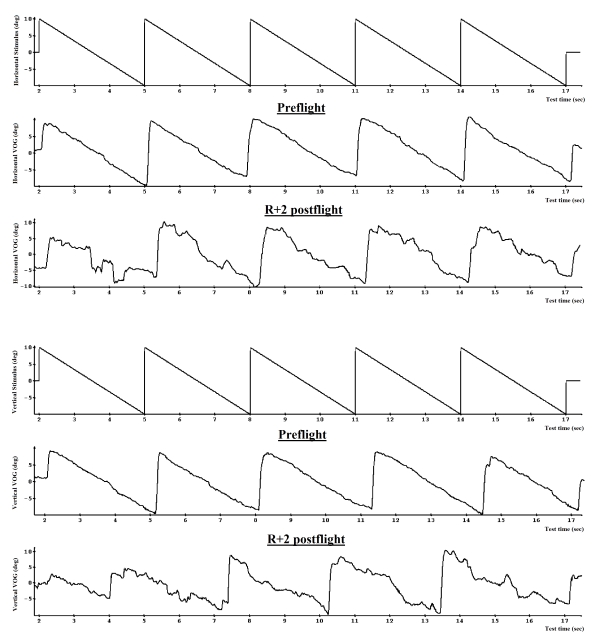
Fig. 11. Dynamic saccades and linear smooth pursuit before and after spaceflight (VOG)
Table 1. Visual tracking parameters before and after spaceflight
| Parameters | Фон | R+1(2) | R+4(5) | R+8(9) |
| М ± σ CV |
М ± σ CV |
М ± σ CV |
М ± σ CV |
|
| Horizontal | ||||
| Latency, sec | 0.28 ± 0.05 17.86% |
0.32 ± 0.05 * 15.63% |
0.30 ± 0.05 16.67% |
0.28 ± 0.05 17.86% |
| Efficiency ratio of FS (eFS) | 0.97 ± 0.03 3.09% |
0.72 ± 0.10 * ↓ 13.89% * |
0.81 ± 0.07 * ↑ 8.64% * |
0.93 ± 0.07 * ↑ 7.53% * |
| Peak velocity of FS, deg/sec | 377.8 ± 18.2 4.81% |
301.8 ± 82.2 * 27.22% * |
312.8 ± 88.3 * 28.24% * |
315.3 ± 61.0 * 19.34% * |
| Percentage of corrective saccades, % | 3.27 ± 3.53 | 18.55 ± 8.40 * ↑ | 12.50 ± 5.98 * ↓ | 6.73 ± 4.83 * ↓ |
| Gain of SP (gSP) | 0.94 ± 0.05 5.32% |
0.70 ± 0.12 * ↓ 17.14% * |
0.83 ± 0.11 * ↑ 13.25% * |
0.82 ± 0.14 * 17.07% * |
| Vertical | ||||
| Latency, sec | 0.26 ± 0.05 19.23% |
0.35 ± 0.06 * 17.14% |
0.30 ± 0.05 ↓ 16.67% |
0.27 ± 0.05 18.52% |
| Efficiency ratio of FS (eFS) | 0.94 ± 0.04 4.26% |
0.68 ± 0.06 * ↓ 8.82% * |
0.75 ± 0.09 * ↑ 12.00% * |
0.92 ± 0.05 ↑ 5.43% |
| Peak velocity of FS, deg/sec | 368.6 ± 18.5 5.03% |
261.3 ± 59.3 * 22.70% * |
347.8 ± 99.2 * ↑ 28.52% * |
343.0 ± 88.3 * 25.73% * |
| Percentage of corrective saccades, % | 6.18 ± 3.35 | 30.65 ± 9.63 * ↑ | 21.00 ± 6.30 * ↓ | 11.18 ± 5.22 ↓ |
| Gain of SP (gSP) | 0.94 ± 0.05 5.32% |
0.69 ± 0.16 * ↓ 23.19% * |
0.73 ± 0.13 * 17.81% * |
0.95 ± 0.08 ↑ 8.42% |
M – mean (average value), σ – standard deviation, CV – coefficient of variation
* – a significant difference from baseline value, p < 0,05
↑ or ↓ – a significant difference (increase or decrease) in comparison with previous eximination (for example, R+1-2 and R+4-5), p < 0,05
Gaze holding (GH) on a real or imaginary target
The reaction of gaze-holding on a real (visible) and imaginary target (visual stimulus) was tested before and after long-term exposure to weightlessness. GH study was performed in a fully darkened room and a monitor equipped with a special optical filter was used for stimulus presentation.
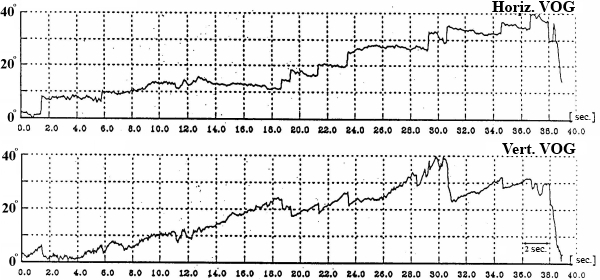
Preflight, cosmonauts fulfilled the GH test quite well. Postflight, gaze nystagmus, the so-called gaze-evoked nystagmus was registered during the gaze holding on an eccentric imaginary target (Fig. 12).
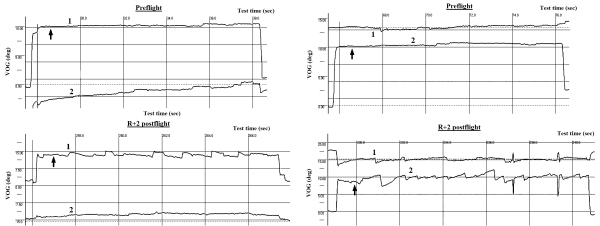
Fig. 12. Gaze holding on a real (visible) and imaginary target before and after spaceflight:
1 – horizontal VOG, 2 – vertical VOG
↑ – time of target’ (stimulus) disappearance
Postflight, parameters of GH were significantly reduced, especially during the initial phase of readaptation. Regain of baseline values of such parameters as time of gaze holding, amplitude and number of corrective saccades was not observed even on R+8(9) (Table 2).
Table 2. Parameters of GH before and after spaceflight
| Parameter | Baseline | R+1(2) | R+4(5) | R+8(9) |
| М ± σ | М ± σ | М ± σ | М ± σ | |
| Horizontal | ||||
| Time of gaze holding, sec | 5.21 ± 1.29 | 2.93 ± 1.61 * ↓ | 3.84 ± 1.67 * | 3.20 ± 1.04 * |
| Number of corrective saccades | 2 ± 1 | 5 ± 2 * ↑ | 3 ± 1 * ↓ | 3 ± 2 * |
| Amplitude of corrective saccades, deg | 1.30 ± 0.56 | 2.89 ± 0.87 * ↑ | 2.56 ± 0.65 * | 2.12 ± 0.74 * ↓ |
| Amplitude of gaze drift, deg | 0.80 ± 0.31 | 2.21 ± 0.65 * ↑ | 1.47 ± 0,89 * ↓ | 0.98 ± 0.45 ↓ |
| Vertical | ||||
| Time of gaze holding, sec | 4.52 ± 1.11 | 1.31 ± 0.57 * ↓ | 1.89 ± 0.83 * | 2.20 ± 0.86 * |
| Number of corrective saccades | 2 ± 1 | 9 ± 2 * ↑ | 8 ± 3 * | 5 ± 2 * ↓ |
| Amplitude of corrective saccades, deg | 1.07 ± 0.73 | 3.75 ± 1.01 * ↑ | 2.79 ± 0.85 * ↓ | 1.32 ± 0.41 ↓ |
| Amplitude of gaze drift, deg | 1.21 ± 0.64 | 2.98 ± 1.05 * ↑ | 1.81 ± 0.89 * ↓ | 1.08 ± 0.95 ↓ |
M – mean (average value), σ – standard deviation, CV – coefficient of variation
* – a significant difference from baseline value, p < 0,05
↑ or ↓ – a significant difference (increase or decrease) in comparison with previous eximination (for example, R+1-2 and R+4-5), p < 0,05
Effect of vestibular and tactile-support afferentation on the visual tracking in microgravity
Vestibular stimulation by active head rotation improved parameters of SpEM, SP and FS significantly in all cosmonauts. After active head movements parameters of FS were improved and amplitude of saccades almost reached the baseline; eFS increased from 0.7 to 1.0 for horizontal plane and from 0.4 to 0.7 for vertical one. Vestibular stimulation recovered the structure of SP reflex and increased gSP.
Additional tactile-support afferentation (ATSA) was taken positively by the majority of cosmonauts who subjectively recognized that they felt better, especially at the begining of spaceflight. However, analysis made with disregard for spatial orientation did not show any quantitative evidence of the effects of ATSA on visual tracking in microgravity. Based on answers in the questionnaire at the beginning of spaceflight, the cosmonauts were distributed into 2 categories: 58% developed their perception of space and own positioning using exclusively visual cues and 34% of cosmonauts relied on internal body coordinates (top and down were defined by the position of legs and head). The first group was classed as the visual orientation type and the latter as the postural orientation type. Analysis of the ATSA showed that visual tracking of a small foveal stimulus was improved only in those cosmonauts (34%) who formed their spatial perception with reference to internal body coordinates (postural type).
Conceptual model of neurosensory mechanisms of space adaptation syndrome (SAS)
In- and postflight changes of oculomotor reactions both spontaneous and induced by vestibular and visual stimulation evidence for a development of the central reinterpretation of sensory stimuli in microgravity that provides the ability to retain a stable image on the retina.
In- and postflight sensorimotor disorders which are phenomenologically identical are the direct results of sensory shifts and ensuing sensory adaptation/readaptation. Process of adaptive changes in the system of intersensory interactions consists of two parallel processes, i.e. disintegration of old intersensory connections developed in the course of evolution, and integration of new ones to provide an adequate existence in weightlessness.
Spatial illusions, disorientation, atypical sensorimotor reactions at the beginning of spaceflight and on the initial phase of postflight readaptation are not destiny of individual space travelers but consistent reactions of human sensory systems on transition to altered gravity. These reactions vary with people in their severity, way of manifestation, time of development, duration and dynamics of adaptation/readaptation processes. The recorded individual differences of reactions in the vestibular system and intersensory interactions stem from inherent or acquired patterns of the functioning of sensory systems and different rates of adaptation processes.
In the early period of adaptation to weightlessness, vestibulae-oculomotor disorders are reflex by nature. Changes in spontaneous eye movements and induced oculomotor reactions that we registered on the initial days of spaceflight point, on the one hand, to reduction of tonic (static) vestibular excitability and, on the other, increase of dynamic excitability of the vestibular input. Involvement of peripheral parts of the vestibular system in genesis of atypical oculomotor reactions in microgravity was confirmed by their dependence on the presence of visual input (appearance or intensification of spontaneous nystagmus with eyes closed), and data obtained from primates showing that one of the reasons for oculomotor disturbance is changed excitability of peripheral vestibular structures demonstrated by direct measurement of neuronal activity of the vestibular nerve and vestibular nuclei.
After the reflex mechanisms, sensorimotor disintegration of processing of visual and kinestatic information were engaged. Concurrently changes in spontaneous and induced oculomotor reactions due to the involvement of peripheral and central segments of the vestibular system were registered. Increase in the number of spontaneous eye movements, appearance of spontaneous nystagmus of typical and atypical forms (square wave jerks), less successful gaze holding on a real and imaginary target, gaze nystagmus, use of the new visual tracking strategy (appearance of corrective saccades during gaze fixation, replacement of the smooth pursuit reflex by the saccadic approximation strategy) advocate for participation of the central mechanisms of the vestibular system and reflect alterations in functioning of vestibular nuclei, nuclei of reticular formation, midbrain tegmentum and vestibulocerebellum (flocculus, nodulus, uvula and paraflocculus). Engagement of the cerebellum in adaptation/readaptation processes is beyond question because of registration of many pseudoclinical cerebellum syndromes.
The mechanism of sensorimotor disintegration included also sensory deprivation. Significance of the deficit of vestibular afferentation in microgravity was confirmed by weakening of the spontaneous nystagmus and improvement of the visual tracking following a series of active head movements. However, microgravity may affect functions of the otolith and semicircular canals directly and also indirectly, removing support and minimizing proprioceptive afferentation, through central integrative multisensory structures of the CNS that converse afferent inputs of various modality (primarily visual, vestibular, support and locomotion). The role of support afferentation in realization of vestibular reflexes and accuracy of visual tracking was demonstrated convincingly in dry immersion experiments.
Recorded asymmetry of the oculomotor response to vestibular and visual stimulation invite consideration of the concept according to which disturbance of the paired function of labyrinths contributes to the development of disorders observed in cosmonauts during adaptation/readaptation.
To summarize, the mechanism of sensory disintegration includes activation of dynamic vestibular-ocular reactions through inhibition of tonic vestibular excitability, development of sensory deprivation due to reduction of the afferent flow from gravity receptors, development of interlabyrinths asymmetry and inter-nuclei disbalance. Sensory disintegration also means breakdown of an evolutionally formed stereotype of intersensory relations (destruction of the 1-g “nervous sensory support model”).
Since the vestibular system is a key player in realization of all types of oculomotor reactions responsible for accuracy of tracking of visual objects, the above changes in the vestibular function during the adaptation/readaptation cannot fail to affect the visual tracking which was demonstrated in the studies of visually-induced oculomotor reactions.
Dramatic changes in the activities of gravity-dependent sensory systems which are critical for accuracy of visual tracking lead not only to a greater variability and significant degradation of all parameters of visual tracking, but also to changing of the tracking strategy. Inaccuracy of saccadic and smooth tracking, along the vertical plane specifically, and establishment of another tracking strategy when gaze approaches target or follows it by series of saccadic movements result in a substantial (in 2.5-3 times) extension of time needed to recognise a visual target and to fixate gaze upon it.
Along with sensory disintegration other adaptation processes occurred to identify an afferent flow that would be relatively reliable in the new environment. This brings about suppression of the vestibular afferent inputs and blockage of unusual for the CNS vestibular information; in the meantime, information coming from the visual input become prevailing. Starting from 60-day of spaceflight (sometimes 30 day) all data obtained point to growing importance of the visual input and a secondary role of the vestibular afferentation in formation of the oculomotor response. This decline of reactivity up to a full functional “arreactivity” of the vestibular system was a result of central inhibition of transmitting to effector mechanisms vestibular signals inadequate to the new conditions: no nystagmus was registered during active head rotation; vestibular reactions to combined vestibular-optokinetic stimulation were very rare whereas optokinetic reactions were more intensive. The phenomenon of inversion of vection illusion during OKS presentation in microgravity is another evidence for prevalence of the visual input.
That is changes of the role of different sensory inputs in integrated reactions of organism, the so-called redistribution of roles, was a reflection of adaptation to the novel sensory environment. Adaptation to microgravity was based on selective activities of the CNS relay and control parts and building up of new intersensory relations. All these adjustments were aimed at re-establishment of central integrative mechanisms that would control reactions on a new functional level adequate to the microgravity environment. Functioning of the vestibular-oculomotor system on a new level was testified by parameters of the vestibular function and visual tracking in the period of compensation which differed from preflight values though still remained within the physiological norm. The period of compensation was characterized by construction in the CNS of a new “nervous agravitational sensory support model” to ensure adequate realization of altered vestibular afferentation in the unusual life conditions. However, as studies in long-term spaceflights showed, the new “nervous model” was rather precarious and vulnerable to additional adverse factors. After 60 days in microgravity, atypical spontaneous and induced by visual and vestibular stimulation oculomotor responses began to appear once and again. Therefore, changes in the vestibular and related sensory systems were transitory throughout long-term spaceflights, i.e. the period of adaptation dominance gave way to readaptation dominance (decompensation).
In summary, the diversity of disorders in spontaneous, vestibular- and visually-induced oculomotor reactions registered during and after spaceflight witness involvement of all the levels of vestibular and oculomotor innervation mechanisms which are responsible to generation of these oculomotor reactions.